AMNIOTIC FLUID AMBOLISM:
Definition:
Amniotic fluid embolism is a rare but serious condition that occurs when amniotic fluid — the fluid that surrounds a baby in the uterus during pregnancy — or fetal material, such as fetal cells, enters the mother's bloodstream. Amniotic fluid embolism is most likely to occur during delivery or in the immediate postpartum period.
Description:
Amniotic fluid embolism is difficult to diagnose. If your doctor suspects you might have one, you'll need immediate treatment to prevent potentially life-threatening complications.
Symptoms
Amniotic fluid embolism might develop suddenly and rapidly. Signs and symptoms might include:
- Sudden shortness of breath
- Excess fluid in the lungs (pulmonary edema)
- Sudden low blood pressure
- Sudden failure of the heart to effectively pump blood (cardiovascular collapse)
- Life-threatening problems with blood clotting (disseminated intravascular coagulopathy)
- Bleeding from the uterus, cesarean incision or intravenous (IV) sites
- Altered mental status, such as anxiety or a sense of doom
- Chills
- Rapid heart rate or disturbances in the rhythm of the heart rate
- Fetal distress, such as a slow heart rate, or other fetal heart rate abnormalities
- Seizures
- Loss of consciousness
Causes
Amniotic fluid embolism occurs when amniotic fluid or fetal material enters the mother's bloodstream. A likely cause is a breakdown in the placental barrier, such as from trauma.
When this breakdown happens, the immune system responds by releasing products that cause an inflammatory reaction, which activates abnormal clotting in the mother's lungs and blood vessels. This can result in a serious blood-clotting disorder known as disseminated intravascular coagulation.
However, amniotic fluid embolisms are rare — and it's likely that some amniotic fluid commonly enters the mother's bloodstream during delivery without causing problems. It's not clear why in some mothers this leads to amniotic fluid embolism.
Risk factors
It's estimated that there are between one and 12 cases of amniotic fluid embolism for every 100,000 deliveries. Because amniotic fluid embolisms are rare, it's difficult to identify risk factors.
Research suggests that several factors might be linked to an increased risk of amniotic fluid embolism, however, including:
- Advanced maternal age. If you're 35 or older at the time of your child's birth, you might be at increased risk of amniotic fluid embolism.
- Placenta problems. Abnormalities in the placenta — the structure that develops in your uterus during pregnancy — might increase your risk of amniotic fluid embolism. Abnormalities might include the placenta partially or totally covering the cervix (placenta previa) or the placenta peeling away from the inner wall of the uterus before delivery (placental abruption). These conditions can disrupt the physical barriers between you and your baby.
- Preeclampsia. Having high blood pressure and excess protein in your urine after 20 weeks of pregnancy (preeclampsia) can increase your risk.
- Medically induced labor. Limited research suggests that certain labor induction methods are associated with an increased risk of amniotic fluid embolism. Research on this link, however, is conflicting.
- Operative delivery. Having a C-section, a forceps delivery or a vacuum extraction might increase your risk of amniotic fluid embolism. These procedures can disrupt the physical barriers between you and your baby. It's not clear, however, whether operative deliveries are true risk factors for amniotic fluid embolism because they're used after the condition develops to ensure a rapid delivery.
- Polyhydramnios. Having too much amniotic fluid around your baby may put you at risk of amniotic fluid embolism.
Complications
Amniotic fluid embolism can cause serious complications for you and your baby, including:
- Brain injury. Low blood oxygen can cause permanent, severe neurological damage or brain death.
- Lengthy hospital stay. Women who survive an amniotic fluid embolism often require treatment in the intensive care unit and — depending on the extent of their complications — might spend weeks or months in the hospital.
- Maternal death. The number of women who die of amniotic fluid embolism (mortality rate) is very high. The numbers vary, but as many as 20 percent of maternal deaths in developed countries may be due to amniotic fluid embolisms.
- Infant death. Your baby is at risk of brain injury or death. Prompt evaluation and delivery of your baby improves survival.
Diagnosis
A diagnosis of amniotic fluid embolism is typically made after other conditions have been ruled out.
Your health care provider might order the following lab tests during your evaluation:
- Blood tests, including those that evaluate clotting, heart enzymes, electrolytes and blood type, as well as a complete blood count (CBC)
- Electrocardiogram (ECG or EKG) to evaluate your heart's rhythm
- Pulse oximetry to check the amount of oxygen in your blood
- Chest X-ray to look for fluid around your heart
- Echocardiography to evaluate your heart's function
Treatment
Amniotic fluid embolism requires rapid treatment to address low blood oxygen and low blood pressure.
Emergency treatments might include:
- Catheter placement. A thin, hollow tube placed into one of your arteries (arterial catheter) might be used to monitor your blood pressure. You might also have another tube placed into a vein in your chest (central venous catheter), which can be used to give fluids, medications or transfusions, as well as draw blood.
- Oxygen. You might need to have a breathing tube inserted into your airway to help you breathe.
- Medications. Your doctor might give you medications to improve and support your heart function. Other medications might be used to decrease the pressure caused by fluid going into your heart and lungs.
- Transfusions. If you have uncontrollable bleeding, you'll need transfusions of blood, blood products and replacement fluids.
If you have amniotic fluid embolism before delivering your baby, your doctor will treat you with the goal of safely delivering your baby as soon as possible. An emergency C-section might be needed.
Coping and support
Experiencing a life-threatening pregnancy condition can be frightening and stressful for you and your family. Afterward, you might relive the experience and have nightmares and flashbacks.
During this challenging time, lean on loved ones for support. Consider joining a survivors' network. Also, work with your health care provider to determine how you can safely manage your recovery and your role as the mother of a newborn.
DILATION AND CURETTAGE (D&C)
Definition:
Dilation and curettage (D&C) is a procedure to remove tissue from inside your uterus. Doctors perform dilation and curettage to diagnose and treat certain uterine conditions — such as heavy bleeding — or to clear the uterine lining after a miscarriage or abortion.
Description:
In a dilation and curettage — sometimes spelled "dilatation" and curettage — your doctor uses small instruments or a medication to open (dilate) your cervix — the lower, narrow part of your uterus. Your doctor then uses a surgical instrument called a curette to remove uterine tissue. Curettes used in a D&C can be sharp or use suction.
Why it's done
Dilation and curettage can diagnose or treat a uterine condition.
To diagnose a condition
Your doctor might recommend a type of D&C called endometrial sampling to diagnose a condition if:
- You have abnormal uterine bleeding
- You experience bleeding after menopause
- Your doctor discovers abnormal endometrial cells during a routine test for cervical cancer
To perform the test, your doctor collects a tissue sample from the lining of your uterus (endometrium) and sends the sample to a lab for testing. The test can check for:
- Endometrial hyperplasia — a precancerous condition in which the uterine lining becomes too thick
- Uterine polyps
- Uterine cancer
To treat a condition
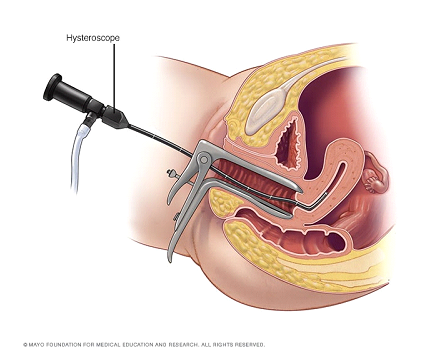
HysteroscopyOpen pop-up dialog box
When performing a therapeutic D&C, your doctor removes the contents from inside your uterus, not just a small tissue sample. Your doctor may do this to:
- Clear out tissues that remain in the uterus after a miscarriage or abortion to prevent infection or heavy bleeding
- Remove a molar pregnancy, in which a tumor forms instead of a normal pregnancy
- Treat excessive bleeding after delivery by clearing out any placenta that remains in the uterus
- Remove cervical or uterine polyps, which are usually noncancerous (benign)
Your doctor may perform the D&C along with another procedure called a hysteroscopy. During a hysteroscopy, your doctor inserts a slim instrument with a light and camera on the end into your vagina, through your cervix and up into your uterus.
Your doctor then views the lining of your uterus on a screen, noting any areas that look abnormal, making sure there aren't any polyps and taking tissue samples as needed. During a hysteroscopy, your doctor can also remove uterine polyps and fibroid tumors
Risks
Dilation and curettage is usually very safe, and complications are rare. However, there are risks. These include:
- Perforation of the uterus. Perforation of the uterus occurs when a surgical instrument pokes a hole in the uterus. This happens more often in women who were recently pregnant and in women who have gone through menopause.
- Most perforations heal on their own. However, if a blood vessel or other organ is damaged, a second procedure may be necessary to repair it.
- Damage to the cervix. If the cervix is torn during the D&C, your doctor can apply pressure or medicine to stop the bleeding, or can close the wound with stitches (sutures).
- Scar tissue on the uterine wall. Rarely, a D&C results in development of scar tissue in the uterus, a condition known as Asherman's syndrome. Asherman's syndrome happens most often when the D&C is done after a miscarriage or delivery.
This can lead to abnormal, absent or painful menstrual cycles, future miscarriages and infertility.
- Infection. Infection after a D&C is possible, but rare.
Contact your doctor if you experience any of the following after a D&C:
- Bleeding that's heavy enough that you need to change pads every hour
- Fever
- Cramps lasting more than 48 hours
- Pain that gets worse instead of better
- Foul-smelling discharge from the vagina
How you prepare
Dilation and curettage may be performed in a hospital, clinic or your doctor's office, and it's usually done as an outpatient procedure.
Before the procedure:
- Follow your doctor's instructions on limiting food and drink.
- Arrange for someone to help you get home because you may be drowsy after the anesthesia wears off.
- Clear your schedule to allow enough time for the procedure and recovery afterward. You'll likely spend a few hours in recovery after the procedure.
In some cases, your doctor may start the process of dilating your cervix a few hours or even a day before the procedure. This helps your cervix open gradually and is usually done when your cervix needs to be dilated more than in a standard D&C, such as during pregnancy terminations or with certain types of hysteroscopy.
To promote dilation, your doctor uses a medication called misoprostol (Cytotec) — given orally or vaginally — to soften the cervix or inserts a slender rod made of laminaria into your cervix. The laminaria gradually expands by absorbing the fluid in your cervix, causing your cervix to open.
What you can expect
During the procedure
Open pop-up dialog box_1658723560.PNG)
Dilation and curettage (D&C)Open pop-up dialog box
For dilation and curettage, you'll receive anesthesia. The choice of anesthesia depends on the reason for the D&C and your medical history.
General anesthesia makes you unconscious and unable to feel pain. Other forms of anesthesia provide light sedation or use injections to numb only a small area (local anesthesia) or a larger region (regional anesthesia) of your body.
During the procedure:
- You lie on your back on an exam table while your heels rest in supports called stirrups.
- Your doctor inserts an instrument called a speculum into your vagina, as during a Pap test, in order to see your cervix.
- Your doctor inserts a series of thicker and thicker rods into your cervix to slowly dilate your cervix until it's adequately opened.
- Your doctor removes the dilation rods and inserts a spoon-shaped instrument with a sharp edge or a suction device and removes uterine tissue.
Because you're either unconscious or sedated during a D&C, you shouldn't feel any discomfort.
After the procedure
You may spend a few hours in a recovery room after the D&C so that your doctor can monitor you for heavy bleeding or other complications. This also gives you time to recover from the effects of anesthesia.
If you had general anesthesia, you may become nauseated or vomit, or you might have a sore throat if a tube was placed in your windpipe to help you breathe. With general anesthesia or light sedation, you may also feel drowsy for several hours.
Normal side effects of a D&C may last a few days and include:
- Mild cramping
- Spotting or light bleeding
For discomfort from cramping, your doctor may suggest taking ibuprofen (Advil, Motrin IB, others) or another medication.
You should be able to resume your normal activities within a day or two.
Wait to put anything in your vagina until your cervix returns to normal to prevent bacteria from entering your uterus, possibly causing an infection. Ask your doctor when you can use tampons and resume sexual activity.
Your uterus must build a new lining after a D&C, so your next period may not come on time. If you had a D&C because of a miscarriage, and you want to become pregnant, talk with your doctor about when it's safe to start trying again.
Results
Your doctor will discuss the results of the procedure after the D&C or at a follow-up appointment.